Болезнь Пейрони
Болезнь Пейрони - индурация фибропластическая полового члена (лат. induratio - затвердение, уплотнение, fibra - волокно), заболевание с преимущественной локализацией патологического процесса в пещеристых телах полового члена, приводящее к его деформации во время эрекции.
Что такое болезнь Пейрони
Среди заболеваний мужской половой системы болезнь Пейрони занимает одно из ведущих мест, несмотря на свою незначительную распространенность - от 0,3 до 1 %.
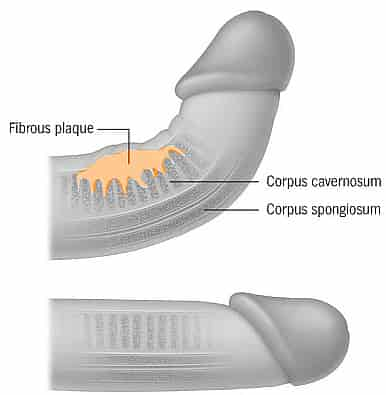
Болезнь Пейрони, или фибропластическая индурация полового члена, характеризуется образованием плотных бляшек в белочной оболочке кавернозных тел, приводящих к возникновению болезненных эрекций, искривлению пениса при эрекции, уменьшению его ригидности, что приводит к сексуальной неудовлетворенности и глубокой психологической травме.
Впервые детально это состояние описал Francois Gigot de la Peyronie - основатель Парижской хирургической академии, который в 1743 году наблюдал трех пациентов с "четковидной рубцовой тканью, последствием чего явилось искривление пениса, направленное вверх, во время эрекции". Болезнь Пейрони чаще всего поражает мужчин в возрасте 40-60 лет, средний возраст - 53 года, но иногда встречается у мужчин более старшего или молодого возраста. Этиология и патогенез настоящего заболевания во многом еще не ясны. В настоящее время большое значение уделяется микротравмам белочной оболочки. Предполагается, что кровоизлияния в ней, возникающие вследствие разрывов тонких кровеносных сосудов, в последующем фиброзно перерождаются с отложением солей кальция. Гистогенез, клинические проявления фибропластической индурации полового члена имеют много общего с патологическими процессами, относящимися к группе коллагенозов. Все исследователи, начиная с Peyronie, Wesson, Rovinesco, Wegenknecht, Kolle, и др. рассматривают болезнь Пейрони как полиэтиологичное заболевание, роль в развитии которого играют травматический, воспалительный, генетический и иммунологический факторы.
Наиболее распространенные симптомы болезни Пейрони - наличие пальпируемой бляшки -78-100%, искривление полового члена - 52-100%, болезненные эрекции - 70%. Размеры бляшек колеблются от нескольких миллиметров до нескольких сантиметров и в среднем составляют 1,5 - 2 сантиметра. В зависимости от локализации бляшки различают дорсальное, вентральное и латеральное искривление полового члена.
Методы лечения болезни Пейрони
В XIX веке для лечения болезни Пейрони использовались йод, мышьяк, камфора. Позднее для этой цели стали использовать радиотерапию, коротковолновую диатермию, лазерную терапию и литотрипсию. Пероральная терапия стала применяться с 1948 года, когда Scott и Scardino начали использовать витамин Е (токоферола ацетат) для лечения болезни Пейрони. Katz-Galatzi, Chauvin и Silvan использовали этот препарат как самостоятельно, так и для комплексной терапии. С другой стороны Ashworth и Bystrom сообщили о неэффективности применения токоферолов, однако витамин Е применяется и в настоящее время. Также для лечения болезни Пейрони использовались биогенные стимуляторы и ферменты - лидаза, ронидаза, тиомуказа, которые применялись как парентерально, так и местно - путем инъекции или электрофореза.
Gelbard и соавт. исследовали влияние ферментов на соединительную ткань как здоровую, так и патологически измененную; в обоих случаях происходило растворение коллагеновых волокон, однако не была уточнена доза препарата для воздействия только на пораженный участок белочной оболочки. Также, у ферментных препаратов существует существенный недостаток - иммунный ответ, вплоть до анафилактического шока. Ralth и соавт. описали опыт применения перорального тамоксифена в 1992 году. Предварительное исследование показало обнадеживающие результаты у пациентов с небольшой давностью заболевания - менее 4 месяцев. Режим приема - 20 мг тамоксифена 2 раза в день в течение 3 месяцев. 80 % пациентов сообщили о снижении болевого симптома, 35 % - уменьшение деформации, 34 % отмечали сокращение объема бляшки. Пероральная терапия колхицином была описана в открытом исследовании Akkus и соавт. Это вещество повышает активность коллагеназы и тем самым уменьшает синтез коллагена. В результате у 11% испытуемых незначительно регрессировало искривление пениса, а у 26% наблюдалось выраженное уменьшение эректильной деформации. В 1954 году Tesley для терапии болезни Пейрони предложил пероральное и местное применение стероидов, основываясь на их противовоспалительных свойствах. Однако осложнение при местном применении стероидов (выраженный болевой симптом, образование микрогематом и участков повторного фиброза) ограничивали широкое использование этого метода.
Winter и Khanna в 1954 году опубликовали результаты своего исследования эффективности местных инъекций дексаметазона (Dermo-jet). Было отмечено уменьшение размера бляшки и болей при эрекции, но не было выявлено статистически достоверной разницы по сравнению с группой контроля. Однако в дальнейшем этот метод получил широкое распространение. В 1980 году Williams и Green сообщили об использовании триамцинолона (местные инъекции). В этом исследовании был описано наблюдение, не включенное в официальный доклад, когда у пациента развилась надпочечная недостаточность, из-за чрезмерного употребления стероидных инъекций. Кроме того, инъекции стероидов могут создавать препятствия для дальнейшего хирургического лечения, так как становится очень трудно разделить ткани между фасцией Бука и белочной оболочкой.
Антагонист кальция - верапамил был впервые использован для местного применения в 1994 г. В исследовании принимали участие 27 пациентов, которые прошли полный курс терапии. Субъективно 96% отметили быструю регрессию болевого симптома. Пенильная деформация уменьшилась у 85%, увеличилась, ригидность - у 74% и повысилась сексуальная удовлетворенность в 89% всех случаев. Объективное исследование включало дуплексное ультразвуковое исследование до и после лечения, которое показало уменьшение искривления у 61% со средним значением 220 (10-400). Гринев А.В. и соавт. сообщают об успешном применении верапамила у 11 пациентов с болевым синдромом. Верапамил вводился в фиброзные бляшки в дозировке 10 мг в 10 мл изотонического раствора один раз в две недели до 10 сеансов. В результате болевой симптом купировался у всех больных, в том числе и у пациента с кальцификацией фиброзных бляшек, в среднем после четвертой процедуры. Уменьшение размеров бляшек наблюдалось в среднем на 40%, исключая вышеуказанного пациента. Степень искривления полового члена снизилась в среднем на 35%.
Для лечения болезни Пейрони используется множество физиотерапевтических методов - рентгенотерапия, радиотерапия, хотя сейчас ее применение ограничено из-за большого числа побочных эффектов (ожоги, изъязвления кожи, эректильная дисфункция, нарушение функции половых желез, развитие метаплазии мезенхимальных клеток, из которых в дальнейшем развивается фиброзная, хрящевая, а затем костная ткань бляшки). В литературе описано применение электронного пучка, диадинамических токов, диатермии, грязелечения, электрофореза гистамина, лидазы, глюкокортикоидов, гелий-неонового лазера.
Хорошие результаты отмечены при применении ультразвуковой терапии, механизм которой основан на ускорении биохимических реакций и вибрационном массаже тканей. Применяется также сочетание ультразвукового метода лечения с нанесением на бляшку лекарственных препаратов (бутадион, гидрокортизон, витамин Е). Большинство авторов отмечает хороший обезболивающий эффект лечения, отсутствие побочных эффектов, уменьшение размеров фиброзной бляшки у некоторых больных. Однако полного рассасывания бляшки и регрессии искривления пениса ни у одного пациента не было отмечено.
Такие препараты, как аминопропионитрил (ингибитор коллагеновых связей), интерфероны, орготеин (противовоспалительный металлопротеин), паратиреоидный гормон находятся в I и II фазах клинических испытаний, и об эффективности и безопасности применения данных препаратов и веществ еще рано говорить. Эффективность консервативной терапии невысока и положительные результаты отмечаются у 10-25% пациентов, но, несмотря на это, многие авторы указывают на необходимость применения консервативной терапии как монотерапии, так и в комбинации с оперативными методами лечения.
При отсутствии эрекции половой член обычной конфигурации. Во время эрекции происходит его искривление, что сопровождается появлением умеренных болей в половом члене, исчезающих вместе с эрекцией. В некоторых случаях резкая деформация органа и боли вообще исключают половой контакт. Постепенно снижается либидо и способность к эрекции, что тяжело переживается больным и нередко приводит к формированию невротических состояний.
Диагноз фибропластической индурации полового члена не представляет трудности, поскольку хрящевидные уплотнения легко прощупываются на тыльной поверхности. Однако для выяснения степени распространения процесса, состояния пещеристых тел и окружающих бляшки соседних тканей в некоторых случаях применяют рентгенологические и ультразвуковые методы исследования. Сечение заболевания длительное. Возможно лечение в период формирования бляшек общим воздействием на организм и местным воздействием на очаги индурации, включающим в себя введение витаминов, десенсибилизирующих средств, биостимуляторов, гормонов, рассасывающих препаратов (непосредственно в очаг). Физиотерапевтические процедуры также предупреждают развитие уплотнений и способствуют рассасыванию.
В период стабилизации рубцового процесса, когда отчётливо проявляется искривление полового члена, необходимы приспособительные навыки ведения полового акта (подбор позы и положения, а также петтинговая подготовка партнёрши для сокращения времени достижения ею оргазма).
В случаях безуспешности консервативного лечения или нестабильности его эффекта показано оперативное лечение. Прогноз даже после хирургического лечения не всегда благоприятный, поскольку заболевание склонно к рецидивам.
Чтобы оставить комментарий , Вам необходимо Авторизоваться или пройти Регистрацию